You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
FMJ for self defense
- Thread starter Guv
- Start date
filthy phil
New member
I would in. 45
would rather not in a 9
would rather not in a 9
Gabe Saurez has some interesting points to the issue here.....I would in. 45
would rather not in a 9
http://www.three-peaks.net/CaliberChoice01.pdf
"One of my contacts in South America has a score of 47...many of those with a Glock 17 with Military FMJ. He prevailed by being generous with his trigger and accurate in his shooting. Good enough for me. For me, its a 9mm Glock 17 with alot of Corbon DPX rounds.
Modern Technique schools created a cult of the 1911/45 and believe that it would work 19 times out of 20. Yet, Fairbairn, a man who was operational in the same general era as Cooper, states that one man he knew emptied his 45 into a thug whom he had to club into unconsciousness with the empty pistol after he kept fighting. So much for legendary stopping power.
That is not to say the 45 is worthless, as it is certainly not. If I was limited by foolish laws to 10 rounds or less, or to FMJ ammo, I might opt for such a pistol, but I think the lack of capacity is a serious limitation.
I investigated an attempted suicide once where a man shot himself in the head with a 1911. He lived and walked out of the ER. What does that prove? Nothing other than the 1911/45 is NOT the death ray excalibur its cultists would have us all assume.
I was also present in an entry where a drug dealer was kiled with one shot from a Sig P226/9mm +P+ 115 gr JHP. The man fell before the Point Man could hit him again. What does that prove? That the 9mm is not the POS, or the "45 set on stun" MT people like to call it.
For perspective I also saw several gang killings with 22 pistols. No lack of stopping power there.
In my educated and experienced opinion, ALL handgun calibers will do about the same things in flesh. I have had ER docs tell me directly that it is impossible to tell what caliber a bullet is in the ER by the damage it does. We have info of the same things happening with just about every caliber out there. Chuck Taylor told me once of a Viet Cong who got his entire shoulder blown off by a 50 BMG that kept charging until he bled out. So again IMHO, the arguement of the Power Of The Pistol is simply a silly idea.
We carry them for convenience and not for power. The secret to dropping the adversary is not the caliber, it is the volume and the placement. Period."
Another "my buddy" tale & more discourse on a really beat up subject.
ALL bullets can kill people.
I'd rather use h.p. ammo in my 40 & 45s.
Hardball kills people, just look at the stats from any military
conflict.
We are not in a war right here, right now, just yet.
Use what you want as you see best.
ALL bullets can kill people.
I'd rather use h.p. ammo in my 40 & 45s.
Hardball kills people, just look at the stats from any military
conflict.
We are not in a war right here, right now, just yet.
Use what you want as you see best.
I have had ER docs tell me directly that it is impossible to tell what caliber a bullet is in the ER by the damage it does.
WHAT???
You mean to tell me on all the TV shows (CSI, CSI NY, CSI Miami, NCIS, Body of Evidence, Bones, Castle etc.) when the star of the show looks down at the bloody chest of the corpse at the scene of the crime and says 'looks like a 9mm' (not a .38 or .380 but a 9mm) that they are messin' with me?
Oh well, I guess I'll watch 'em anyway.
peacefulgary
New member
The potential of hollow-point expansion is appealing, but shot placement and penetration are key.
If you put the bullets where they count, FMJ can certainly get the job done.
If you put the bullets where they count, FMJ can certainly get the job done.
I wouldn't feel too handicapped with FMJs in a pistol, especially something like a .45 which already has a short stubby bullet, with not much velocity.
With a rifle, I would never opt for non-expanding ammo, unless my opponents were heavily armored for some reason, in which case AP ammo would be the way to go.
Pistols just poke holes.
Expanding bullets poke bigger holes, when they expand, and in return sacrifice penetration.
Bigger holes are more effective for causing bleed out faster.
A .22 cal hole in the stomach that expanded to .31 cal isn't a whole lot worse than a .22 cal hole that goes completely through the target.
OTOH a .43 cal bullet that expands to .70 cal is pretty darn big hole, but it still is just a hole, and if it's not in the right place, it likely wont be that much more effective than a FMJ with the same placement.
I prefer to have exit wounds with my SD loads. FMJ's could do this reliably, but if the cartridge has enough power to create consistent exit wounds with expanding ammo, that would be my preference.
With a rifle, I would never opt for non-expanding ammo, unless my opponents were heavily armored for some reason, in which case AP ammo would be the way to go.
Pistols just poke holes.
Expanding bullets poke bigger holes, when they expand, and in return sacrifice penetration.
Bigger holes are more effective for causing bleed out faster.
A .22 cal hole in the stomach that expanded to .31 cal isn't a whole lot worse than a .22 cal hole that goes completely through the target.
OTOH a .43 cal bullet that expands to .70 cal is pretty darn big hole, but it still is just a hole, and if it's not in the right place, it likely wont be that much more effective than a FMJ with the same placement.
I prefer to have exit wounds with my SD loads. FMJ's could do this reliably, but if the cartridge has enough power to create consistent exit wounds with expanding ammo, that would be my preference.
I've done 7 autopsies myself (under direction of the coroner) and never could tell what caliber was used to shoot the victim.
S.g. wounds are a much, much differen matter. (yuk)
Seen more autopsies done. My job as detective ya know.
Studied many other gun shot autopsies and the only way to determine caliber is by recovered the weapon & better still the bullet too.
S.g. wounds are a much, much differen matter. (yuk)
Seen more autopsies done. My job as detective ya know.
Studied many other gun shot autopsies and the only way to determine caliber is by recovered the weapon & better still the bullet too.
Frank Ettin
Administrator
Sigh! Not again. Consider that there are reasons why today virtually all law enforcement agencies use JHP ammunition.
As I've said before:
There is data, and there are studies, and we have a good deal of knowledge about wound physiology. But we keep getting into these "ring-around-the-rosie" discussions because, I guess, a lot of people are dissatisfied that there really is no definitive answer.
Perhaps the real conclusion(s) with regard to self defense could be summarized as follows:
I've posted the following before and might as well post it again here:
Let's consider how shooting someone will actually cause him to stop what he's doing.
As I've said before:
There is data, and there are studies, and we have a good deal of knowledge about wound physiology. But we keep getting into these "ring-around-the-rosie" discussions because, I guess, a lot of people are dissatisfied that there really is no definitive answer.
Perhaps the real conclusion(s) with regard to self defense could be summarized as follows:
- Pretty much every cartridge ever made has at times succeeded at quickly stopping an assailant.
- Pretty much every cartridge ever made has at times failed at quickly stopping an assailant.
- Considering ballistic gelatin performance, data available on real world incidents, an understanding of wound physiology and psychology, certain cartridges with certain bullets are more likely to be more effective more of the time.
- For defensive use in a handgun the 9mm Luger, .38 Special +P, .40 S&W, .45 ACP, .357 Magnum, and other, similar cartridges when of high quality manufacture, and loaded with expanding bullets appropriately designed for their respective velocities to both expand and penetrate adequately, are reasonably good choices.
- And that's probably as good as we can do.
I've posted the following before and might as well post it again here:
Let's consider how shooting someone will actually cause him to stop what he's doing.
- The goal is to stop the assailant.
- There are four ways in which shooting someone stops him:
- psychological -- "I'm shot, it hurts, I don't want to get shot any more."
- massive blood loss depriving the muscles and brain of oxygen and thus significantly impairing their ability to function
- breaking major skeletal support structures
- damaging the central nervous system.
Depending on someone just giving up because he's been shot is iffy. Probably most fights are stopped that way, but some aren't; and there are no guarantees.
Breaking major skeletal structures can quickly impair mobility. But if the assailant has a gun, he can still shoot. And it will take a reasonably powerful round to reliably penetrate and break a large bone, like the pelvis.
Hits to the central nervous system are sure and quick, but the CNS presents a small and uncertain target. And sometimes significant penetration will be needed to reach it.
The most common and sure physiological way in which shooting someone stops him is blood loss -- depriving the brain and muscles of oxygen and nutrients, thus impairing the ability of the brain and muscles to function. Blood loss is facilitated by (1) large holes causing tissue damage; (2) getting the holes in the right places to damage major blood vessels or blood bearing organs; and (3) adequate penetration to get those holes into the blood vessels and organs which are fairly deep in the body. The problem is that blood loss takes time. People have continued to fight effectively when gravely, even mortally, wounded. So things that can speed up blood loss, more holes, bigger holes, better placed holes, etc., help.
So as a rule of thumb --
- More holes are better than fewer holes.
- Larger holes are better than smaller holes.
- Holes in the right places are better than holes in the wrong places.
- Holes that are deep enough are better than holes that aren't.
- There are no magic bullets.
- There are no guarantees.
- psychological -- "I'm shot, it hurts, I don't want to get shot any more."
- With regard to the issue of psychological stops see
- this study by Greg Ellifritz. And take special notice of his data on failure to incapacitate rates:
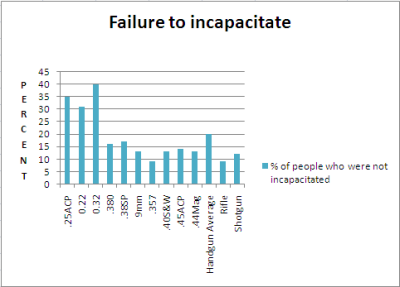
As Ellifritz notes in his discussion of his "failure to incapacitate" data (emphasis added):Greg Ellifritz said:...Take a look at two numbers: the percentage of people who did not stop (no matter how many rounds were fired into them) and the one-shot-stop percentage. The lower caliber rounds (.22, .25, .32) had a failure rate that was roughly double that of the higher caliber rounds. The one-shot-stop percentage (where I considered all hits, anywhere on the body) trended generally higher as the round gets more powerful. This tells us a couple of things...
In a certain (fairly high) percentage of shootings, people stop their aggressive actions after being hit with one round regardless of caliber or shot placement. These people are likely NOT physically incapacitated by the bullet. They just don't want to be shot anymore and give up! Call it a psychological stop if you will. Any bullet or caliber combination will likely yield similar results in those cases. And fortunately for us, there are a lot of these "psychological stops" occurring. The problem we have is when we don't get a psychological stop. If our attacker fights through the pain and continues to victimize us, we might want a round that causes the most damage possible. In essence, we are relying on a "physical stop" rather than a "psychological" one. In order to physically force someone to stop their violent actions we need to either hit him in the Central Nervous System (brain or upper spine) or cause enough bleeding that he becomes unconscious. The more powerful rounds look to be better at doing this....
- There are two sets of data in the Ellifritz study: incapacitation and failure to incapacitate. They present some contradictions.
- Considering the physiology of wounding, the data showing high incapacitation rates for light cartridges seems anomalous.
- Furthermore, those same light cartridges which show high rates of incapacitation also show high rates of failures to incapacitate. In addition, heavier cartridges which show incapacitation rates comparable to the lighter cartridges nonetheless show lower failure to incapacitate rates.
- And note that the failure to incapacitate rates of the 9mm Luger, .40 S&W, .45 ACP, and .44 Magnum were comparable to each other.
- If the point of the exercise is to help choose cartridges best suited to self defense application, it would be helpful to resolve those contradictions.
- A way to try to resolve those contradictions is to better understand the mechanism(s) by which someone who has been shot is caused to stop what he is doing.
- Considering the physiology of wounding, the data showing high incapacitation rates for light cartridges seems anomalous.
- The two data sets and the apparent contradiction between them (and as Ellifritz wrote) thus strongly suggest that there are two mechanisms by which someone who has been shot will be caused to stop what he is doing.
- One mechanism is psychological. This was alluded to by both Ellifritz and FBI agent and firearms instructor Urey Patrick. Sometimes the mere fact of being shot will cause someone to stop. When this is the stopping mechanism, the cartridge used really doesn't matter. One stops because his mind tells him to because he's been shot, not because of the amount of damage the wound has done to his body.
- The other mechanism is physiological. If the body suffers sufficient damage, the person will be forced to stop what he is doing because he will be physiologically incapable of continuing. Heavier cartridges with large bullets making bigger holes are more likely to cause more damage to the body than lighter cartridges. Therefore, if the stopping mechanism is physiological, lighter cartridges are more likely to fail to incapacitate.
- One mechanism is psychological. This was alluded to by both Ellifritz and FBI agent and firearms instructor Urey Patrick. Sometimes the mere fact of being shot will cause someone to stop. When this is the stopping mechanism, the cartridge used really doesn't matter. One stops because his mind tells him to because he's been shot, not because of the amount of damage the wound has done to his body.
- And in looking at any population of persons who were shot and therefore stopped what they were doing, we could expect that some stopped for psychological reasons. We could also expect others would not be stopped psychologically and would not stop until they were forced to because their bodies became physiologically incapable of continuing.
- From that perspective, the failure to incapacitate data is probably more important. That essentially tells us that when Plan A (a psychological stop) fails, we must rely on Plan B (a physiological stop) to save our bacon; and a heavier cartridge would have a lower [Plan B] failure rate.
- There are two sets of data in the Ellifritz study: incapacitation and failure to incapacitate. They present some contradictions.
- this study by Greg Ellifritz. And take special notice of his data on failure to incapacitate rates:
- Also see the FBI paper entitled "Handgun Wounding Factors and Effectiveness", by Urey W. Patrick. Agent Patrick, for example, notes on page 8:...Psychological factors are probably the most important relative to achieving rapid incapacitation from a gunshot wound to the torso. Awareness of the injury..., fear of injury, fear of death, blood or pain; intimidation by the weapon or the act of being shot; or the simple desire to quit can all lead to rapid incapacitation even from minor wounds. However, psychological factors are also the primary cause of incapacitation failures.
The individual may be unaware of the wound and thus have no stimuli to force a reaction. Strong will, survival instinct, or sheer emotion such as rage or hate can keep a grievously wounded individual fighting.... - And for some more insight into wound physiology and "stopping power":
- Dr. V. J. M. DiMaio (DiMaio, V. J. M., M. D., Gunshot Wounds, Elsevier Science Publishing Company, 1987, pg. 42, as quoted in In Defense of Self and Others..., Patrick, Urey W. and Hall, John C., Carolina Academic Press, 2010, pg. 83):In the case of low velocity missles, e. g., pistol bullets, the bullet produces a direct path of destruction with very little lateral extension within the surrounding tissue. Only a small temporary cavity is produced. To cause significant injuries to a structure, a pistol bullet must strike that structure directly. The amount of kinetic energy lost in the tissue by a pistol bullet is insufficient to cause the remote injuries produced by a high-velocity rifle bullet.
- And further in In Defense of Self and Others... (pp. 83-84, emphasis in original):The tissue disruption caused by a handgun bullet is limited to two mechanisms. The first or crush mechanism is the hole that the bullet makes passing through the tissue. The second or stretch mechanism is the temporary wound cavity formed by the tissue being driven outward in a radial direction away from the path of the bullet. Of the two, the crush mechanism is the only handgun wounding mechanism that damages tissue. To cause significant injuries to a structure within the body using a handgun, the bullet must penetrate the structure.
- And further in In Defense of Self and Others... (pp. 95-96, emphasis in original):Kinetic energy does not wound. Temporary cavity does not wound. The much-discussed "shock" of bullet impact is a fable....The critical element in wounding effectiveness is penetration. The bullet must pass through the large blood-bearing organs and be of sufficient diameter to promote rapid bleeding....Given durable and reliable penetration, the only way to increase bullet effectiveness is to increase the severity of the wound by increasing the size of the hole made by the bullet....
- Dr. V. J. M. DiMaio (DiMaio, V. J. M., M. D., Gunshot Wounds, Elsevier Science Publishing Company, 1987, pg. 42, as quoted in In Defense of Self and Others..., Patrick, Urey W. and Hall, John C., Carolina Academic Press, 2010, pg. 83):
- And sometimes a .357 Magnum doesn't work all that well. LAPD Officer Stacy Lim who was shot in the chest with a .357 Magnum and still ran down her attacker, returned fire, killed him, survived, and ultimately was able to return to duty. She was off duty and heading home after a softball game and a brief stop at the station to check her work assignment. According to the article I linked to:... The bullet ravaged her upper body when it nicked the lower portion of her heart, damaged her liver, destroyed her spleen, and exited through the center of her back, still with enough energy to penetrate her vehicle door, where it was later found....
- But take special note of the quote in the third bullet point in item V., above:
- In In Defense of Self and Others... (pp. 95-96, with my emphasis):... the only way to increase bullet effectiveness is to increase the severity of the wound by increasing the size of the hole made by the bullet....
- And that leads us to prefer expanding bullets.
- In In Defense of Self and Others... (pp. 95-96, with my emphasis):

nc-oldfart
New member
There is NO condition I would use a round nosed fmj bullet. There are cartidges that may be better with swc designs like a slow cartidges where a standard velocity HP may not expand or if dealing with heavier clothing. 200gr 45 driven hard would far better than any round nose . Most 380 loads would be better as a 100 to 105gr swc if any heavy clothing is in the mix and the handgun will cycle them reliably.
i would not use fmj for defense
I've watched some youtube vids recently of fmj 9mm and 45 acp zipping right through ballistics gel. I consider that to be of major concern in any situation where there may be other people around.
I'll take hollow points please.
Fmj
http://www.youtube.com/watch?v=3G-txVKnVjY
http://www.youtube.com/watch?v=mNfp2LtfTHc
Hp
http://www.youtube.com/watch?v=bqziWTq7X1c
These videos are worth your consideration
I've watched some youtube vids recently of fmj 9mm and 45 acp zipping right through ballistics gel. I consider that to be of major concern in any situation where there may be other people around.
I'll take hollow points please.
Fmj
http://www.youtube.com/watch?v=3G-txVKnVjY
http://www.youtube.com/watch?v=mNfp2LtfTHc
Hp
http://www.youtube.com/watch?v=bqziWTq7X1c
These videos are worth your consideration