@ JohnKSa
Yes, once an X-Ray negative has been exposed, it's not possible to make the sort of adjustment I did if you're dealing exclusively with the film. And, even with the sort of adjustment possible with computer manipulation, an improperly exposed and/or developed negative may still not show some thing that CAN be shown if the exposure and development process are managed correctly. (Like the SilverTip Jacket in this case. Although, I think if you do an actual overlay of the visible and X-Ray images, I think you will find that it is nearly all visible.)
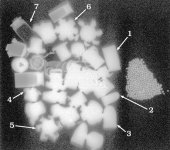
It is not. That grey halo around the bullet is not the jacket it is an anomaly associated with the lead core outline and the filter that has been applied to the image. How do I know? Because the same halo is seen associated with bullet No 3 which is an all-lead bullet. If you applied the above observation to that bullet too, you would falsely arrive at the conclusion that the bullet was jacketed. All of the high density items in your manipulated image have that grey halo, even brass cartridge bases. In fact all of them have also lost radiographic density from white to grey. This, like the mottle, is a misrepresentation of the densities on the radiograph. There are no exposure factors that can create that false representation. It is entirely due to your manipulation.
Whoever took that X-Ray and developed it did not do so with an eye to detecting aluminum and therefore the aluminum showed up VERY poorly in some cases and not at all in other cases.
I took the radiograph, and actually the converse is true. I took it specifically to image jacketing. I used the lowest radiographic exposure that we currently used in that department at the time, which is the exposure used to X-ray hands/fingers. The film/screen combination was the highest detail available in the department. It was a fine grain film with a fine grain phosphor intensifying screen. Even if we could go lower, we would not be justified to apply a non-diagnostic dose to the patient. In other words you can't justify doing a really soft X-ray exposure on a person on the off-chance that there is a piece of aluminium jacketing in a gunshot wound. It doesn't work that way. Resources wouldn't permit it even if the radiation concern was ignored. If you wanted to prospectively detect those pieces of aluminium and you had time and resources to burn, then ultrasound would be a better modality. We don't alter the X-ray exposure for forensic purposes, the exposure is always governed by clinical need.
I have shown that X-Rays CAN show aluminum, as I stated in my eariler post, and what's more, I did it with your picture. Furthermore, as a pointed out earlier, it only takes a little work with an internet search engine to show that aluminim is faintly radio-opaque and that it is even used to calibrate X-rays--something that would not be possible if it were invisible.
Yes you have shown that parts of the cartirdge case can be rendered visible under extreme and non-available/not permitted manipulation of the radiograph. If you want me to apologise to you about that, I will: here it is, I screwed up. I did not take into account the fact that the cartridge case was constructed of an aluminium alloy which would be detectable upon aggressive manipulation of my radiograph by you, JohnSKa. You showed me the cartridge case when I thought you wouldn't be able to. Does it change anythng in the world of diagnostic radiography? No, it doesn't, because in day-to-day radiography where you are X-raying anatomy there is no way you will see that. Bear in mind a cartridge case is quite big compared to a bullet jacket. Aluminium step wedges: I was the first to concede in this thread that a sizeable piece of aluminium will be seen on X-ray. I was the first to mention step wedges. If you look at a quality control film that has had a wedge exposed on it, the first step or two of aluminium are not detectable on film, and those are quite thick steps, certainly thicker than anything you would find in a projectile component. Thats why they use that step wedge: to get a range of densities from black to white. There isn't another metal you can do that with. Clearly aluminium is special in that it cannot be detected easily like other metals (and I contend that in small quantities and in the pieces of projectile fragments I have seen, it is not detectable at all with current radiography standards).
There is no way you will convince me. In the first place, I just posted an X-Ray with aluminum visible on it. You may not like how I did it, but clearly your assertion that aluminum is invisible on X-Rays is incorrect based solely on that picture.
Actually, objectively I have to agree with you. I should have been more specific about the contribution of other metals in aluminium alloys to produce a radio-opaque shadow on the film. The use of that cartridge case in this debate has been a poor choice for me. I will have to find out what its metallurgical composition is. But note that it would not have been seen in hospital viewing conditions. It is not a projectile component either. But that's a point (when argued the way you have set out above) that you must win.
If that weren't enough, it only takes a little bit of internet search to confirm that aluminum is indeed visible on X-Rays. I can post a bunch of links if you want, but given that you're balking at the picture, it seems a waste of my time.
That is not a waste of time, it just isn't relevant because it depends on which alloys of aluminium you are talking about. I think I said that in my response to Guntotin Fool above when he mentioned auto aluminium.
The film was not properly exposed and developed to detect aluminum. It was exposed and developed to show details in the VERY dense lead objects and therefore the aluminum was washed out. My manipulation showed that the aluminum is visible, but because of the way the X-ray was initially made and developed, the results were not ideal.
I used a standard hand protocol for that radiograph. In that hospital, the exposure is 50kV and 2.5mAs. It is the most
unsuitable exposure to use to image lead. It is a very low exposure. That is why you can see the copper-based jackets in good detail. You cannot see any lead detail because the X-ray beam at that kVp is incapable of passing through lead. There could be a massive air bubble in all of those bullets and you wouldn't know because the X-ray beam at that kVp is stopped by the smallest thickness of lead. In fact the beam has not even been able to penetrate the bases of the brass cartridge cases. In terms of the development of the radiograph, that is automatic these days in just about every hospital you go to. Nobody dips films anymore. You don't get a processor-related change in density that is under the user's control. There is nothing wrong with the processing.
It's likely that the manipulation would yield far better results if there were only overlying/surrounding anatomy. The problem with the X-Ray as it stands is that the VERY dense lead is monopolizing the dynamic range and washing out the aluminum. With only much less dense soft tissue as a background, the aluminum would be far more easily visible.
It has nothing to do with lead monopolising anything. No density being radiographed can 'wash out' an adjacent one. In fact there is no such thing as washout in radiography. Washout applies to photography. You can't blame my radiograph for the effects of your manipulation. I have told you already, your manipulation provides a false representation of the actual densities of the items being radiographed. If this isn't the case, then how do you explain the grey halos around all the items, even the cartridge case above bullet 6 (there is no lead in that case)?
Now you've proved that some aluminium alloys can be seen in extreme circumstances. But these aren't the circumstances that apply to trauma radiography today. Even the radiograph I have posted is not indicative of the film/screen combinations employed today in the emergency room. Typical exposure values for chests and abdomens start at 70kV with 4mAs and can run to 90kV with mAs values up to 40, depending on the kV selected. At those exposures you can even miss copper-based jacketing, but you can still see tissue outlines. You can see the effects of kV increment on step wedges. At those kVs you might find that the first 4 or 5 steps of the wedge cannot be seen.
I am unmoved. Based on my knowledge of X-ray exposure factors and the appearance of projectile components in gunshot wounds I adhere to my previous statement that aluminium projectile components will not be visible on X-rays done in the hospital setting. I am still willing to prove this to anyone who doubts it. If you would like to send me your aluminium fragments I will insert those into the appropriate media and X-ray them with a range of exposures. You can have the original radiographs and tell me which ones have visible aluminium.
")