You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Bullets hitting bone?
- Thread starter CobrayCommando
- Start date

CobrayCommando
Moderator
Amazing X-rays and awesome information, thanks Odd Job!
Thanks everybody for contributing. I now know that sternum shots are unlikely to produce large amounts of bone fragmentation when hit by service caliber handgun bullets.
I'm guessing the same holds for rifle bullets... But then again...
Thanks everybody for contributing. I now know that sternum shots are unlikely to produce large amounts of bone fragmentation when hit by service caliber handgun bullets.
I'm guessing the same holds for rifle bullets... But then again...
@ epr105
No, my good man, not to that extent any way. All these images are from South Africa, as is my experience. I trained in South Africa and worked three years permanent night duty at the Johannesburg General Hospital at a time when we were getting an average of 150 gunshot victims a month. And just to 'add sauce to the meal' I followed that up with formal research into gunshot wounds in 2002, tracing the victim from the time he was admitted through all the treatment and imaging, surgery (if applicable), recovery of any projectiles (if applicable) and documenting the acute recovery prognosis. That was a sample of 150 patients and required 450 data sheets and resulted in 1600 photographs of wounds, clothing breaches, X-rays/medical imaging and recovered projectiles. That sample is the subject of a book I am writing (almost finished) and so I can't post those pictures here for copyright reasons. But I have 'adequate' experience and imaging from my years before the research. Some of my older articles are on FirearmsID.com if you are interested in the subject of forensics and gunshot wounds.
I hope that puts my contributions on a more solid footing, in your eyes
I see your location is London. Please tell me are people still shooting each other in the gun free UK?
No, my good man, not to that extent any way. All these images are from South Africa, as is my experience. I trained in South Africa and worked three years permanent night duty at the Johannesburg General Hospital at a time when we were getting an average of 150 gunshot victims a month. And just to 'add sauce to the meal' I followed that up with formal research into gunshot wounds in 2002, tracing the victim from the time he was admitted through all the treatment and imaging, surgery (if applicable), recovery of any projectiles (if applicable) and documenting the acute recovery prognosis. That was a sample of 150 patients and required 450 data sheets and resulted in 1600 photographs of wounds, clothing breaches, X-rays/medical imaging and recovered projectiles. That sample is the subject of a book I am writing (almost finished) and so I can't post those pictures here for copyright reasons. But I have 'adequate' experience and imaging from my years before the research. Some of my older articles are on FirearmsID.com if you are interested in the subject of forensics and gunshot wounds.
I hope that puts my contributions on a more solid footing, in your eyes
I must add (to avoid future confusion) that I am not a doctor, I am a radiographer. But as Long Path knows, Johannesburg is definitely the place to see gunshot wounds. Many foreign doctors go down there to get trauma experience and I would like to think that I have bailed most of them out in terms of interpreting imaging in gunshot cases at one time or another. In fact in cases such as those I have posted here, there is a clinical as well as forensic advantage to tracking the path of these projectiles and any bone fragments that may be involved. That's why even the local veteran trauma surgeons will not scoff at the input of an experienced radiographer: they are certainly well respected in the medical field in South Africa. I may post examples of a clinical nature (where the bone fragment/fracture pattern has enabled the radiographer to influence further imaging requests to find an as-yet unseen projectile).
Jack O'Conner
New member
When I was a lad, my Grandad always told me, "Go for bone,boy". My first three elk were knocked over with his antique Winchester 30-30. All animals were shot in the shoulder-to-neck joint and their front legs folded as the shot(s) echoed across the foothills. Tremendous energy is transferred to the animal when a large bone is struck!
Grandad always hunted with his medium velocity rifles and heavy bullets, a good combination for bone targets. In contrast, the modern high powered rifle kills as well with shot placement behind-the-shoulder.
I saw several dead Iraqi soldiers during Gulf War Part I that had been killed with the dimunitive 5.56mm bullet(s). Exit wounds had the appearance of soft tip hunting ammo but caused by high velocity, tumbling, and bone fragments. I have never actually shot at anyone, my AFSC was combat support.
Jack
Grandad always hunted with his medium velocity rifles and heavy bullets, a good combination for bone targets. In contrast, the modern high powered rifle kills as well with shot placement behind-the-shoulder.
I saw several dead Iraqi soldiers during Gulf War Part I that had been killed with the dimunitive 5.56mm bullet(s). Exit wounds had the appearance of soft tip hunting ammo but caused by high velocity, tumbling, and bone fragments. I have never actually shot at anyone, my AFSC was combat support.
Jack
@ Long Path
X-rays aren't a problem, but there are several issues surrounding wound photographs:
1) More than 90% of my wound photographs are from the research I conducted and are subject to copyright. I might be able to get around publishing problems by cropping them and making them B&W. I will have to look into this. I don't have a publisher yet, but the general rules should be applicable to all of them.
2) Most of the photographs were taken with a specially-adapted camera that had a ruler mounted 14cm from the lens. These are close-ups and their position on the body is denoted by a separate 3D figure specially made for each case. So all you will see is a hole of some description, with a scale underneath in millimetres.
3) The entrance and exit wounds from handguns are remarkably similar and often cannot be distinguished in the actively-bleeding victim. Furthermore the surface wounds usually provide no further clue or information about the damage to the internal tissues and bone. I would go so far as to say that of all the photographs, the wound photographs of a live gunshot victim are the least helpful in terms of clinical and forensic information. I rate clothing higher than wounds in terms of projectile tracking.
However, not to be a spoilsport I will provide for you now a gunshot leg with a fractured bone and the accompanying wound photographs. I ask TFL members to respect my work and therefore not distribute these images for although I don't envisage them to be part of the published product I must maintain good relations with those in the publishing field and those who have overseen my research. I will post them soon.
X-rays aren't a problem, but there are several issues surrounding wound photographs:
1) More than 90% of my wound photographs are from the research I conducted and are subject to copyright. I might be able to get around publishing problems by cropping them and making them B&W. I will have to look into this. I don't have a publisher yet, but the general rules should be applicable to all of them.
2) Most of the photographs were taken with a specially-adapted camera that had a ruler mounted 14cm from the lens. These are close-ups and their position on the body is denoted by a separate 3D figure specially made for each case. So all you will see is a hole of some description, with a scale underneath in millimetres.
3) The entrance and exit wounds from handguns are remarkably similar and often cannot be distinguished in the actively-bleeding victim. Furthermore the surface wounds usually provide no further clue or information about the damage to the internal tissues and bone. I would go so far as to say that of all the photographs, the wound photographs of a live gunshot victim are the least helpful in terms of clinical and forensic information. I rate clothing higher than wounds in terms of projectile tracking.
However, not to be a spoilsport I will provide for you now a gunshot leg with a fractured bone and the accompanying wound photographs. I ask TFL members to respect my work and therefore not distribute these images for although I don't envisage them to be part of the published product I must maintain good relations with those in the publishing field and those who have overseen my research. I will post them soon.
CobrayCommando
Moderator
Cooolllll....
john in jax
New member
Just like to add one more tidbit to this excellent thread.
I head-shot a hog at approx 50 yards with a .308 150grn Ballistic Tip. A good shot about midway between the ear and eye. There was no exit wound and since this was the first game I had taken with this round I was curious so I dug around to try and find what was left of the bullet. The obvious wound channel was only about 3"-4" deep but I never found the bullet or any significant fragments. It was as if the bullet disentigrated on impact.
I head-shot a hog at approx 50 yards with a .308 150grn Ballistic Tip. A good shot about midway between the ear and eye. There was no exit wound and since this was the first game I had taken with this round I was curious so I dug around to try and find what was left of the bullet. The obvious wound channel was only about 3"-4" deep but I never found the bullet or any significant fragments. It was as if the bullet disentigrated on impact.
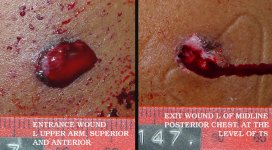
Okay everybody I can't use the leg case because it includes the testicles and that makes photographs awkward. I have however found a gunshot upper arm. The victim was a middle-aged female and the circumstances of the shooting are that multiple shots were fired and the victim was hit once. She was then pushed to the ground and beaten about the head before the assailant ran away. There was no clothing available for inspection.
(Image not embedded in case some people don't like blood)
http://www.thefiringline.com/forums/attachment.php?attachmentid=17301&stc=1&d=1138834268
The orientation of the above photographs is correct if one imagines that the victim was standing when photographed ie. north on the image is north in reality. The scale is in millimetres. Note that both wounds were actively bleeding and the patient was photographed supine.
Now for the radiographs:

This is the L humerus with a nasty fracture. Bone fragments and small lead fragments drift from lateral to medial (parallel to the red arrow) and there is a bullet fragment that has a low density attachment (black arrow) indicating that this bullet is jacketed. The rest of the bullet is high density in appearance which means it is a lead core (white arrow).

This is the chest X-ray. It is difficult to appreciate here but there is a cortical disruption on the lateral border of the scapula (black arrow). For the non-medical folk that means the shoulder blade was nicked on its outside edge. Lead specks can be seen deposited in the wound medial to this disruption (white arrows) and this supports a trajectory parallel to the red arrow.
What can we tell from this? Well the lady was relatively lucky, because what has happened here is that the bullet has shattered the humerus and it has broken into at least two main pieces (the bullet that is). One piece stayed in the region of the axilla (the armpit) and the other hit the scapula edge-on. Now the lucky part is that this second bullet fragment (that was never recovered) could have been deflected anteriorly towards the lung, heart or aorta but instead it was deflected posteriorly where it caused insignificant damage in the region of the thorax. The unlucky thing about this case is that the bullet fragment you see there completely severed the axillary artery and the lady had no pulse in her hand. Plus she had a very nasty fracture that could only be fixed with an external fixator (those Robocop-style rods and pins that look so awkward). So overall the damage was significant but a life-threatening injury was avoided by chance. Something else of interest is when you consider both radiographs as a unit, there is an angled trajectory that doesn't make much sense because the trajectory changes in the axilla for no apparent reason. You can have deflections in tissue planes but a more likely explanation is that the victim's arm was raised at the time of the shooting.
Outcome: the axillary artery was repaired and the humerus was realigned with an external fixator. You may not have thought that so much goes on underneath the skin when there are just two simple-looking holes on the surface of a gunshot victim.
(Image not embedded in case some people don't like blood)
http://www.thefiringline.com/forums/attachment.php?attachmentid=17301&stc=1&d=1138834268
The orientation of the above photographs is correct if one imagines that the victim was standing when photographed ie. north on the image is north in reality. The scale is in millimetres. Note that both wounds were actively bleeding and the patient was photographed supine.
Now for the radiographs:
This is the L humerus with a nasty fracture. Bone fragments and small lead fragments drift from lateral to medial (parallel to the red arrow) and there is a bullet fragment that has a low density attachment (black arrow) indicating that this bullet is jacketed. The rest of the bullet is high density in appearance which means it is a lead core (white arrow).
This is the chest X-ray. It is difficult to appreciate here but there is a cortical disruption on the lateral border of the scapula (black arrow). For the non-medical folk that means the shoulder blade was nicked on its outside edge. Lead specks can be seen deposited in the wound medial to this disruption (white arrows) and this supports a trajectory parallel to the red arrow.
What can we tell from this? Well the lady was relatively lucky, because what has happened here is that the bullet has shattered the humerus and it has broken into at least two main pieces (the bullet that is). One piece stayed in the region of the axilla (the armpit) and the other hit the scapula edge-on. Now the lucky part is that this second bullet fragment (that was never recovered) could have been deflected anteriorly towards the lung, heart or aorta but instead it was deflected posteriorly where it caused insignificant damage in the region of the thorax. The unlucky thing about this case is that the bullet fragment you see there completely severed the axillary artery and the lady had no pulse in her hand. Plus she had a very nasty fracture that could only be fixed with an external fixator (those Robocop-style rods and pins that look so awkward). So overall the damage was significant but a life-threatening injury was avoided by chance. Something else of interest is when you consider both radiographs as a unit, there is an angled trajectory that doesn't make much sense because the trajectory changes in the axilla for no apparent reason. You can have deflections in tissue planes but a more likely explanation is that the victim's arm was raised at the time of the shooting.
Outcome: the axillary artery was repaired and the humerus was realigned with an external fixator. You may not have thought that so much goes on underneath the skin when there are just two simple-looking holes on the surface of a gunshot victim.
Attachments


This year I shot a whitetail at about 60 yards. I was using a thompson center omega loaded with 300 gr tc shockwaves and 100 gr. of tripple 7. The round passed through his right shoulder and at least one lung. Then it hit the left shoulder. The bullet was stuck in the bone, and fragments were everywhere. All the musle turned all stringy. He only ran about another 20 yards.
@ H&H
Indeed there are instances where you can radiologically identify certain features of the bullet, depending on the nature of the X-ray view and the condition of the projectile. Here is a basic summary of what you can do with a radiograph if you are familiar with radiological assessment of metallic densities and composite shadows:
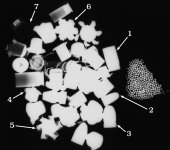
If the bullet is intact or only mildly deformed (relative to its condition when it was loaded in the cartridge) then it is impossible to tell whether it is jacketed or all-lead in construction. The only exception to this is if the design of the bullet is such that the jacket does not appose the core intimately all the way around the projectile. The jacket may then be resolved on the radiograph. The same applies to a bullet with an exposed base: it may have a thickened jacketed 'rim' at the base and if the X-ray beam strikes it at the right angle then the jacket will be detected. But in the majority of cases where the typical handgun bullet shape is seen and there does not appear to be any deformity, it is impossible to say whether that bullet is jacketed or not. I will give you an example of the differences in radiological density as evident in different materials and configurations of a sample of projectiles and projectile components. First the photograph:

Note that most of the bullets were fired in a water tank, but the appearances are consistent with my research as regards the density of projectiles that are retained in the human body. The 9mm bullets have very light rifling impressions because they were fired out of a Vektor CP1 which has polygonal rifling.
1 = semi-jacketed flatnose (.357 mag)
2 = FMJ (.25)
3 = LRN (was oversized bullet loaded in a 9mm cartridge case)
4 = Sentry (9mm 60gn)
5 = Winchester Black Talon (9mm)
6 = Speer Gold Dot (9mm. This is the newer version, don't have gn value at hand)
7 = CCI Blazer Aluminium cartridge case (9mm)
Now look at the radiograph:

Bullets 1-3 have the same radiological density on film and there is no way to tell whether they are semi-jacketed, fully jacketed or not at all jacketed because they are not deformed. The overall high density of the lead obscures the density of the jacketing and the jacketing cannot be resolved.
Bullet number 4 is made from solid copper that is nickel-plated. The expanded rim of this projectile is, in effect, a thin piece of copper and it will show as a low density structure on the radiograph. The main core of the bullet is still very dense and cannot be distinguished from a lead core when discussing the density alone. Of course the bullet has a characteristic shape and the size and configuration of the central post makes it highly suggestive that the bullet is a version of the THV, or BAT or Sentry, but being precise about brand is not wise based on X-ray evidence alone in that case.
Bullet number 5 is a Winchester Black Talon and it has the characteristic 6-petal expansion where the petals are of lower density than the core from which they are separated. If a side view of the projectile is X-rayed and the characteristic barbs are seen then I am happy to conclude that the bullet is a Winchester Black Talon (of unknown calibre) based on the x-ray evidence alone. With that view only, the bullet may be mistaken for a Golden Sabre.
Bullet number six is a Gold Dot (a newer version than the one to the right of it). This is a jacketed bullet but even though the bullet has expanded, the jacket cannot be resolved because it is bonded to the core in such a way that apposition is maintained. There is no core-jacket separation. However, the configuration of the expansion and the lack of a resolved jacket makes it quite viable for me to conclude based on X-ray evidence alone (and with no further views necessary) that the bullet is a Gold Dot of unknown calibre.
The cartridge case labelled 7 is interesting because it demonstrates that aluminium is radiolucent (cannot be seen on X-ray). The significance of this is that any bullet with aluminium jacketing will appear as a single density on film even if it is fragmented. The jacket will not be detected and the bullet will appear to be lead only.
As a matter of interest, can you detect (by comparing the photograph and the radiograph) the bullet that has an aluminium jacket?
Indeed there are instances where you can radiologically identify certain features of the bullet, depending on the nature of the X-ray view and the condition of the projectile. Here is a basic summary of what you can do with a radiograph if you are familiar with radiological assessment of metallic densities and composite shadows:
If the bullet is intact or only mildly deformed (relative to its condition when it was loaded in the cartridge) then it is impossible to tell whether it is jacketed or all-lead in construction. The only exception to this is if the design of the bullet is such that the jacket does not appose the core intimately all the way around the projectile. The jacket may then be resolved on the radiograph. The same applies to a bullet with an exposed base: it may have a thickened jacketed 'rim' at the base and if the X-ray beam strikes it at the right angle then the jacket will be detected. But in the majority of cases where the typical handgun bullet shape is seen and there does not appear to be any deformity, it is impossible to say whether that bullet is jacketed or not. I will give you an example of the differences in radiological density as evident in different materials and configurations of a sample of projectiles and projectile components. First the photograph:
Note that most of the bullets were fired in a water tank, but the appearances are consistent with my research as regards the density of projectiles that are retained in the human body. The 9mm bullets have very light rifling impressions because they were fired out of a Vektor CP1 which has polygonal rifling.
1 = semi-jacketed flatnose (.357 mag)
2 = FMJ (.25)
3 = LRN (was oversized bullet loaded in a 9mm cartridge case)
4 = Sentry (9mm 60gn)
5 = Winchester Black Talon (9mm)
6 = Speer Gold Dot (9mm. This is the newer version, don't have gn value at hand)
7 = CCI Blazer Aluminium cartridge case (9mm)
Now look at the radiograph:
Bullets 1-3 have the same radiological density on film and there is no way to tell whether they are semi-jacketed, fully jacketed or not at all jacketed because they are not deformed. The overall high density of the lead obscures the density of the jacketing and the jacketing cannot be resolved.
Bullet number 4 is made from solid copper that is nickel-plated. The expanded rim of this projectile is, in effect, a thin piece of copper and it will show as a low density structure on the radiograph. The main core of the bullet is still very dense and cannot be distinguished from a lead core when discussing the density alone. Of course the bullet has a characteristic shape and the size and configuration of the central post makes it highly suggestive that the bullet is a version of the THV, or BAT or Sentry, but being precise about brand is not wise based on X-ray evidence alone in that case.
Bullet number 5 is a Winchester Black Talon and it has the characteristic 6-petal expansion where the petals are of lower density than the core from which they are separated. If a side view of the projectile is X-rayed and the characteristic barbs are seen then I am happy to conclude that the bullet is a Winchester Black Talon (of unknown calibre) based on the x-ray evidence alone. With that view only, the bullet may be mistaken for a Golden Sabre.
Bullet number six is a Gold Dot (a newer version than the one to the right of it). This is a jacketed bullet but even though the bullet has expanded, the jacket cannot be resolved because it is bonded to the core in such a way that apposition is maintained. There is no core-jacket separation. However, the configuration of the expansion and the lack of a resolved jacket makes it quite viable for me to conclude based on X-ray evidence alone (and with no further views necessary) that the bullet is a Gold Dot of unknown calibre.
The cartridge case labelled 7 is interesting because it demonstrates that aluminium is radiolucent (cannot be seen on X-ray). The significance of this is that any bullet with aluminium jacketing will appear as a single density on film even if it is fragmented. The jacket will not be detected and the bullet will appear to be lead only.
As a matter of interest, can you detect (by comparing the photograph and the radiograph) the bullet that has an aluminium jacket?
Attachments

Odd Job,
I'd have to say that the aluminum jacketed bullet is the one just below and to the right of the aluminum case marked #7 ?
Having spent some time in South Africa I can only imagine that you'd see quite a mix of weapons and calibers. Is there a particular weapon or caliber that the average thug prefers to use in South Africa that you are aware of ?
Do you as a medical professional who's studied numerous bullets wounds find one type of bullet/caliber to be a more lethal combination than others?
A vague question I'm sure and probably very difficult to answer. The reason I ask it is I was talking to a retired British SBS sergeant at a shooting school who had a very interesting take on this pistol caliber stuff.
He found that of the three calibers most commonly used in a defensive handgun, 9MM, .40S&W and .45ACP that in his experience there wasn't much difference in there ability to kill or stop a human if the shot didn't hit the CNS.
And that any of the above would stop a human cold if they did hit spine or brain. Makes perfect sense to me.
Thus the British SBS teaches to shoot for the "vital triangle" verses "center of mass" the vital triangle is defined as a line from nipple to nipple forming a triangle with it's tip coming together at the adams apple. This will tend to bring your aim higher than what most of us are taught in your average law enforcement style shooting.
Any thoughts on this subject?
I'd have to say that the aluminum jacketed bullet is the one just below and to the right of the aluminum case marked #7 ?
Having spent some time in South Africa I can only imagine that you'd see quite a mix of weapons and calibers. Is there a particular weapon or caliber that the average thug prefers to use in South Africa that you are aware of ?
Do you as a medical professional who's studied numerous bullets wounds find one type of bullet/caliber to be a more lethal combination than others?
A vague question I'm sure and probably very difficult to answer. The reason I ask it is I was talking to a retired British SBS sergeant at a shooting school who had a very interesting take on this pistol caliber stuff.
He found that of the three calibers most commonly used in a defensive handgun, 9MM, .40S&W and .45ACP that in his experience there wasn't much difference in there ability to kill or stop a human if the shot didn't hit the CNS.
And that any of the above would stop a human cold if they did hit spine or brain. Makes perfect sense to me.
Thus the British SBS teaches to shoot for the "vital triangle" verses "center of mass" the vital triangle is defined as a line from nipple to nipple forming a triangle with it's tip coming together at the adams apple. This will tend to bring your aim higher than what most of us are taught in your average law enforcement style shooting.
Any thoughts on this subject?
The better instructors here in the states also teach hitting the "vital triangle". That's because it works !!...While there is never ending discussion of 9mm vs 40S&W, vs 357 sig vs 45acp all the better ammo is designed to conform to the FBI criteria. So bullet placement is more important than any difference between cartridges ! Nothing substitutes for well placed hits !")
@ H+H
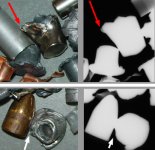
No, it is actually the bullet at 6 o' clock to the right of the FMJ. The bullet you suspected is a 9mm Winchester Silvertip and the base metal of that jacket is copper. See the picture below.

The part of the jacket that is not apposed to the core can be seen on the photograph and the X-ray image (red arrows). The bullet you selected therefore cannot have an aluminium jacket.
The other bullet (the one at 6 o'clock on the original image) is also a Winchester Silvertip but it is .25 calibre and that jacket is made from aluminium. The part of the jacket that is not apposed to the core can only be seen on the photograph, not the X-ray image (white arrrows). To approach the problem from a different direction, think of the angle between that bullet and the FMJ to the left of it, first looking at the photograph. Can you mentally see the same angle on the X-ray image? No. That means the information is missing from the X-ray image (not recorded on film because aluminium is radio-lucent). By the way I have been told that Winchester no longer uses aluminium jacketing. I cannot verify this, but even if this is so, there must be some ammunition out there still in circulation (whether made by Winchester or not) that still has aluminium jacketing.
Yes, the 9mm pistol is the thug's weapon of choice.
I would agree with that.

Well the image above shows the internal anatomy in that triangle. I shaded where I reckon the vital areas are (fast bleedout). The apex of the triangle could result in a paralysis such that the guy can't fire back, but I wouldn't bank on it. That apex is too low to guarantee that the spinal cord will be damaged at a level higher than that at which the nerves to the arms originate. It is a very small target anyway (the spinal cord). Do I reckon it is okay? Yes I think it is, in terms of having the fastest bleedout because it includes the aortic arch and that is more critical than the heart itself in my opinion. I would say that if you can put two shots into that triangle, and the guy isn't too oblique relative to your trajectory, then you have a potentially fatal shooting. And if you miss the triangle there is still 'stuff' around it that can be damaged.
I'd have to say that the aluminum jacketed bullet is the one just below and to the right of the aluminum case marked #7 ?
No, it is actually the bullet at 6 o' clock to the right of the FMJ. The bullet you suspected is a 9mm Winchester Silvertip and the base metal of that jacket is copper. See the picture below.
The part of the jacket that is not apposed to the core can be seen on the photograph and the X-ray image (red arrows). The bullet you selected therefore cannot have an aluminium jacket.
The other bullet (the one at 6 o'clock on the original image) is also a Winchester Silvertip but it is .25 calibre and that jacket is made from aluminium. The part of the jacket that is not apposed to the core can only be seen on the photograph, not the X-ray image (white arrrows). To approach the problem from a different direction, think of the angle between that bullet and the FMJ to the left of it, first looking at the photograph. Can you mentally see the same angle on the X-ray image? No. That means the information is missing from the X-ray image (not recorded on film because aluminium is radio-lucent). By the way I have been told that Winchester no longer uses aluminium jacketing. I cannot verify this, but even if this is so, there must be some ammunition out there still in circulation (whether made by Winchester or not) that still has aluminium jacketing.
Is there a particular weapon or caliber that the average thug prefers to use in South Africa that you are aware of ?
Yes, the 9mm pistol is the thug's weapon of choice.
He found that of the three calibers most commonly used in a defensive handgun, 9MM, .40S&W and .45ACP that in his experience there wasn't much difference in there ability to kill or stop a human if the shot didn't hit the CNS.
I would agree with that.
Nothing is ever certain. Even a spinal hit won't guarantee an instant cessation of activities, particularly if it is the lower cervical vertebrae or any vertebrae in the thoracic or lumbar region.And that any of the above would stop a human cold if they did hit spine or brain. Makes perfect sense to me.
Thus the British SBS teaches to shoot for the "vital triangle" verses "center of mass" the vital triangle is defined as a line from nipple to nipple forming a triangle with it's tip coming together at the adams apple. This will tend to bring your aim higher than what most of us are taught in your average law enforcement style shooting.
Well the image above shows the internal anatomy in that triangle. I shaded where I reckon the vital areas are (fast bleedout). The apex of the triangle could result in a paralysis such that the guy can't fire back, but I wouldn't bank on it. That apex is too low to guarantee that the spinal cord will be damaged at a level higher than that at which the nerves to the arms originate. It is a very small target anyway (the spinal cord). Do I reckon it is okay? Yes I think it is, in terms of having the fastest bleedout because it includes the aortic arch and that is more critical than the heart itself in my opinion. I would say that if you can put two shots into that triangle, and the guy isn't too oblique relative to your trajectory, then you have a potentially fatal shooting. And if you miss the triangle there is still 'stuff' around it that can be damaged.
Attachments

The other bullet (the one at 6 o'clock on the original image) is also a Winchester Silvertip but it is .25 calibre and that jacket is made from aluminium.
Oops, a small mistake there: .25 should read .32
Odd Job, I would like to thank you for the photos and radiographs. As a former pre-med student, this is extremely interesting. And getting information from someone well versed in firearms and forensic science makes this extremely interesting.
My combat experience, although limited due to the nature of the action I was involved in (Grenada 1983), supports much of what has been reported here. My hunting experience is more varied, but a lot of this confirms things I have witnessed over the years.
As for the "vital triangle" concept, it is not unique to SBS or other special forces, and is actually taught in USMC sniper school, albeit under a different name. It is one way experts use to determine if a person was shot by an infantry-trained marksman or a sniper-trained marksman. If there is target movement after the shot, it will likely still result in a lethal hit, with a much higher probability than a head shot. A COM hit will likely result in a non-lethal wound if the target moves or the shot is deflected.
Once again, thank you for sharing the results of your work with us.
My combat experience, although limited due to the nature of the action I was involved in (Grenada 1983), supports much of what has been reported here. My hunting experience is more varied, but a lot of this confirms things I have witnessed over the years.
As for the "vital triangle" concept, it is not unique to SBS or other special forces, and is actually taught in USMC sniper school, albeit under a different name. It is one way experts use to determine if a person was shot by an infantry-trained marksman or a sniper-trained marksman. If there is target movement after the shot, it will likely still result in a lethal hit, with a much higher probability than a head shot. A COM hit will likely result in a non-lethal wound if the target moves or the shot is deflected.
Once again, thank you for sharing the results of your work with us.